- Changing sleep habits in adolescence may be part of normal development.
- Sleep habits, quantity, and quality should be addressed at well child visits.
Renata's Story
Renata is a 15-year-old Hispanic girl who comes to Dr. Marshall’s office for her annual well child check-up. Dr. Marshall has been her pediatrician since birth and has a strong history with the family. The only concern Renata’s mom has is Renata’s sleep habits have changed in the past six months. Renata and her family live in a single-family home in an upper-class neighborhood. Renata has three younger siblings. Renata plays on the soccer team and participates in school plays.
Expert Insights for Changing Sleep Habits
BEARS Screening for Renata
As part of the clinic’s routine protocols all patients are screened with a BEARS assessment tool. Open the categories below to review some of the history that was obtained from Renata's family.
Bedtime Problems
Renata states it usually takes about 15-20 minutes for her to fall asleep after she goes to bed.
Expert Insights
- Normal sleep onset is usually within 20 minutes of going to bed.
Excessive Daytime Sleepiness
Renata sometimes feels sleepy in her class after lunch but doesn’t fall asleep.
Expert Insights
- Sleeping during the day may be an indication of insufficient or abnormal sleep.
Awakenings
Renata denies waking up at night unless she has to go to the bathroom and goes back to sleep without any problems.
Expert Insights
- Frequent nocturnal awakenings and trouble getting back to sleep need further evaluation.
Regularity & Duration
School nights Renata goes to bed at 10:30 PM and gets about 7.5 hours of sleep. Weekends she goes to bed around 11:30 PM and gets about 9 hours of sleep.
Expert Insights
- The American Academy of Sleep Medicine recommends that teens get 8-10 hours of sleep each night.
Sleep-Disordered Breathing / Snoring
Renata snores most nights, according to her mother (although she is infrequently observed at night).
Expert Insights
- Loud snoring with or without apnea may be a symptom of obstructive sleep apnea and needs further evaluation.
Renata's Evaluation & Diagnosis
What evaluation should be recommended to determine if Renata has a sleep problem? Check all that apply and click submit for feedback.
Check all that apply:
The evaluation protocol strategies we recommend for Renata’s case are:
- Determine the child’s sleep history
- Perform a physical exam
- Complete a sleep diary
- Order a Sleep Study
- Interview Adolescent and Parent
- Ask the patient to complete an Epworth Sleepiness Scale
Determine elements of Renata's sleep history
| Sleep History | Case Specific Questions | Renata's Evaluation Results |
|---|---|---|
What the child does at night |
How long is Renata sleeping at night? |
She usually completes her homework about an hour before bedtime. She bathes, organizes her clothes and supplies for the following day while listening to music. |
Review timing of events at night (bedtime/waketime) |
Are Renata’s bedtime and wake up time consistent throughout the week? |
Renata usually goes to bed and awakes at the same time on school nights and goes to bed at least an hour later on weekend nights |
Screen for other sleep issues (OSA, restless leg syndrome) |
Is Renata snoring or pausing in her breathing while sleeping? |
Renata sleeps through the night. Family members do not report that Renata snores. There have been no other sleep related concerns for Renata in the past. |
Review of medications (antidepressants, seizure medications, and antihistamines all have impacts on sleep) |
What medications is Renata taking? |
No prescription or non-prescription medications reported in the past 6 months. |
Is Renata practicing appropriate sleep hygiene? |
|
She has her own room. She stops using her cellphone or laptop one hour before going to bed. There are no known environmental factors that might negatively impact her sleep habits. |
Perform a Physical Exam
| Information to obtain includes: | Case Evaluation Results |
|---|---|
A physical exam should include height, weight, BMI, cardiovascular exam, ENT exam assessing for nasal airway patency and tonsillar size and a thorough neurologic exam. |
Height: 168 cm (75-90%) Weight: 54.5 kg (50-75%) BMI 19.3 kg/m2 (25-50%) Physical exam is normal with 1+ tonsils bilaterally. Normal neurologic examination. |
Complete a Sleep Diary
| Renata's Response: | Renata's Mother Response |
|---|---|
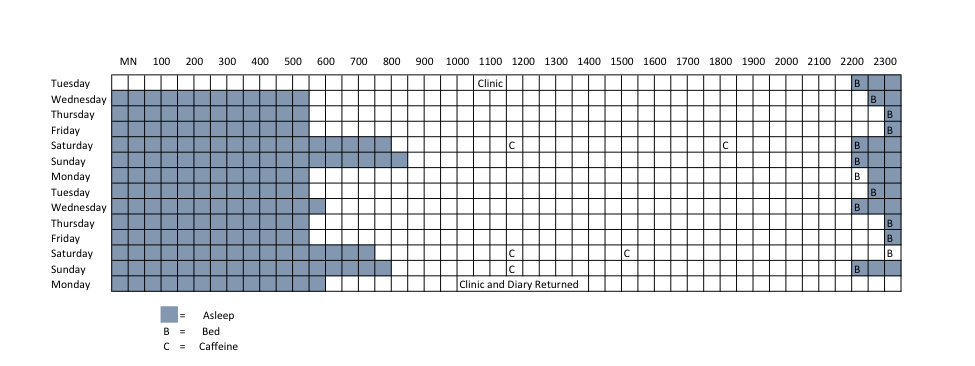
Sleep diaries can provide very useful information to help determine the number of hours that a patient is asleep and in bed. It also allows a visual expression of the patient’s nocturnal and daytime schedule. Sleep diaries are simple and inexpensive and can be used by most families who are experiencing sleep problems. |
Renata’s sleep diary is seen below. 
|
Order a Sleep Study
| Information to obtain includes: | Case Evaluation Results |
|---|---|
A diagnostic polysomnogram is the gold standard for diagnosing sleep-disordered breathing. During the study, respiratory flow, respiratory effort, end tidal CO2 and oxygen levels will be monitored (in addition to other parameters) to determine the presence of sleep-disordered breathing. The sleep study will report an Apnea-Hypopnea Index (AHI, the number of times per hour that the patient pauses breathing or breathes too shallowly while asleep), which is used to diagnose sleep-disordered breathing. In children, an obstructive AHI > 1 event per hour is diagnostic of obstructive sleep apnea. Additionally, if the end tidal CO2 is greater than 50 mmHg for more than 25% of sleep time, this is also considered diagnostic of obstructive sleep apnea. Note that for older children (teenagers), adult scoring criteria may be considered, and an AHI of 5 events per hour may be used as the diagnostic threshold. If possible, the sleep study should be performed at a sleep center with experience managing pediatric patients. This is particularly important for children with neurodevelopmental disabilities, as experienced pediatric technicians will be better equipped to help children feel more comfortable with the procedure. |
Renata completed an overnight sleep study and had light snoring noted. Renata slept well on the night of her sleep study. She had 7.6 hours of sleep recorded and only 3 hypopneas (decreased airflow) on the study. Her apnea-hypopnea index was 0.4. This is normal for age. |
Interview Adolescent and Parent
| Renata's Response: | Renata's Mother Response |
|---|---|
Renata’s responses to separate interview: Renata reports that she is not sexually active, does not smoke, drink alcohol, or take any recreational drugs. She usually drinks one caffeinated soft drink a day. She has one specialty coffee drink two or three times per week after school with her friends. She does not feel that she has any physical or social concerns. Renata states that she follows the rules of no use of electronics one hour before bedtime. Sometimes she has to stay up late to finish a school assignment. She says she falls asleep easily and awakes refreshed and gets busy as soon as she awakes. Renata she is happy and has many friends. |
Renata’s mother’s responses to separate interview: Renata’s mom reports that Renata uses her desk rather than her bed for school projects. Renata follows the family rules of no electronic use one hour before bedtime. Renata has always had good sleep hygiene habits, having the same bedtime and arising at the same time consistently, with exceptions for special occasions. Renata has her own bedroom with attached private bath. When questioned further, the mother notes that Renata is an outstanding student who is already researching colleges she may want to attend. She appears happy and has several really nice friends. To her knowledge Renata does not use any illegal substance nor is she sexually active. In the past few months Renata doesn’t feel sleepy until later at night. On the weekend, she stays up later and wants to sleep in later. She has noticed Renata snoring. |
Ask the patient to complete an Epworth Sleepiness Scale
| Information to obtain includes: | Case Evaluation Results | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
The ESS is a validated instrument that has been used in research studies and clinical applications to quantify the level of sleepiness that a patient is experiencing. The ESS consists of nine scenarios that the respondent is asked about how likely they would be to fall asleep. |
An example of the ESS for Renata is described below: How likely are you to doze off or fall asleep in the following situations, in contrast to just feeling tired? (0=would never doze off, 1=slight chance of dozing off, 2=moderate chance of dozing off, 3=high chance of dozing off).
Renata's ESS is normal for her age. A normal ESS is less than 10. |
Options that are Not Recommended
Refer to a Specialist
A referral to a specialist is not reccomended.
Red Flags
- Screen time (computer, tablet or phone) should end 2 hours before bedtime.
- Avoid exposure to blue light emitted from electronic devices at night. There are apps available to limit blue light exposure.
- Beds should only be used for sleeping not for homework.
- Intake of caffeine and dietary habits can impact sleep quality.
When evaluating a child,
consider how other health care providers may also need to be involved.
Evaluation & Diagnosis
What diagnosis is consistent with Renata’s changing sleep behaviors?
Check all that apply:
Renata’s signs and symptoms are evident of:
- Normal sleep for age and development.
In this case, Renata's sleepiness is not related to obstructive sleep apnea, sleep walking or narcolepsy.
Renata's Treatment & Referrals
Now it’s time to recommend treatment options for Renata.
Check all that apply:
The following treatment strategies are recommended for Renata:
- Educate Renata and her mother about sleep phase delay during puberty.
Typically developing teenagers have a normal delay in their circadian rhythm as puberty occurs. This shift tends to result in teens having a later onset of sleep and a corresponding delay in the optimal awake time. Often teenagers will shift their sleep schedule to later times, but are unable to delay their rise time due to social obligations, such as school. This results in a risk for insufficient sleep for many teenagers.
Consider reviewing healthy sleep habits and normal sleep development. This patient education handout from the American Thoracic Society may be helpful.
- It is not appropriate to refer the patient to ENT as her sleep study did not show evidence of sleep disordered breathing.
- There is no indication to start any medication for Renata’s sleep. Her sleep is normal for age.
Renata's Results:
Good news! Renata and her mother are reassured that this is a normal change in sleep patterns for teenagers called sleep phase delay.